The Discharge Defense System Hospitals Hope You Never Build
The Hospital Discharge Guide is a printable Discharge Defense System — word-for-word appeal scripts, a medication reconciliation audit, "if this then that" decision-tree flowcharts, a 72-hour recovery protocol, and country-specific legal frameworks — that gives you the exact words to say, the exact forms to file, and the exact steps to take when the hospital is rushing your loved one out the door before it's safe. Not a blank planner. Not a 300-page book. Not a government compliance form. A coordinated defense system for the 24 hours between "we're discharging them tomorrow" and the terrifying ride home.
Here's what actually happens: Your parent falls, or has a stroke, or comes out of surgery — and within 48 hours the discharge planner appears with a clipboard and a list of nursing homes you've never heard of. They tell you your parent is "medically stable" and the bed is needed. You haven't slept. You don't know the medication list. Nobody has explained what "medically stable" actually means for someone who can't get to the bathroom alone. The hospital-provided checklist tells you to "ask about complications" but doesn't tell you which complications to expect, what the danger thresholds are, or what to do when nobody answers your questions. You Google for help and get government pamphlets written by the same system that's pushing you out. The free resources exist to protect the hospital's liability. This guide exists to protect your parent.
Covers the US, UK, Canada, Australia, and New Zealand — with country-specific appeal processes, legal rights, regulatory bodies, and post-discharge support systems for each healthcare system.
Is This For You?
This guide is for you — the family member who:
- Just received a discharge notice and has 24-48 hours to figure out how to safely bring a medically fragile parent home — with no training, no equipment, and no plan
- Has been told their loved one is "ready to go" when they can barely stand, can't manage their own medications, and have no home health support arranged
- Wants to appeal the discharge but doesn't know what a QIO is, what BFCC means, or how to file a fast appeal before the deadline expires
- Is terrified their parent will be back in the ER within 72 hours because the hospital sent them home with a medication list that conflicts with what the primary care doctor prescribed
- Has siblings who live far away and can't help — and a job that won't wait — and a healthcare system that treats family caregivers as free, disposable labor
- Needs to know exactly what to say to the discharge planner, the attending physician, and the case manager to legally buy more time — tonight, not after reading a 300-page book
You know the discharge is too soon. The hospital knows it too — but the bed is needed and the algorithm says "medically stable." You need leverage, not sympathy. You need scripts, not pamphlets. You need a Discharge Defense System.
What's Inside the Discharge Defense System
- The 72-Hour Survival Protocol — because the first three nights at home are when preventable readmissions begin. What to monitor every 4 hours, which symptoms demand a doctor call versus an ER trip, and how to set up a medication schedule before the first night home. Designed to be read on a phone screen in a hospital cafeteria.
- Discharge Appeal Scripts — because the hospital counts on you not knowing the magic words. Word-for-word scripts for speaking to the discharge planner, the attending physician, and the patient advocate when the discharge is unsafe. Includes the exact language to invoke the CARE Act (US), request a PALS intervention (UK), file a QIO fast appeal (US Medicare), escalate to the Health and Disability Commissioner (NZ), and trigger a Transition Care Program assessment (Australia). Not "tips for having a conversation" — literal scripts you read from the page.
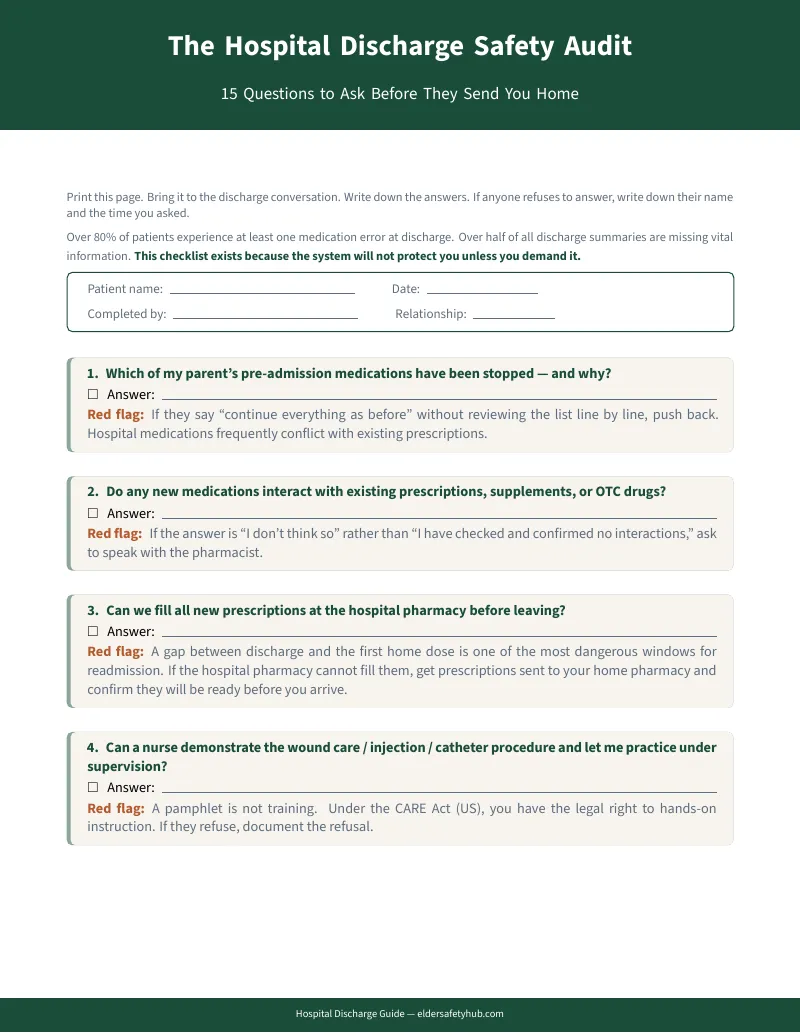
- Medication Reconciliation Audit — because over half of hospital discharge summaries contain medication errors, and nobody warns you. A line-by-line comparison worksheet: every pre-hospital medication next to every new discharge prescription. Flag what changed, verify it with the pharmacist before you leave the building. The document that's supposed to prevent deadly interactions is probably wrong — this worksheet catches the errors before you fill the prescriptions.
- Decision-Tree Flowcharts — because at 2 AM with a spiking fever, you need an answer, not a Google search. Visual "if this, then that" flowcharts for the most dangerous post-discharge scenarios. Fever above 101? Follow the tree. Sudden confusion? Follow the tree. Each flowchart ends with a specific action: call this number, go to the ER, wait and monitor. Tape them to the refrigerator.
- Country-Specific Legal Guide — because your discharge rights differ by country and the hospital won't explain them. US: Medicare fast appeals via the BFCC-QIO, the CARE Act training mandate, observation status vs. inpatient (the billing trap that denies SNF coverage). UK: NHS Discharge to Assess pathways, PALS escalation, Continuing Healthcare funding. Canada: provincial ombudsman contacts, ALC advocacy. Australia: Transition Care Program, My Aged Care triggers. New Zealand: NASC evaluation rights, Te Ara Whakapiri palliative frameworks.
- Home Safety Rapid Assessment — because you have 4 hours between "they're coming home" and the ambulance pulling into the driveway. A room-by-room checklist: trip hazards, grab bars, bed height, bathroom modifications, lighting, medication storage, emergency numbers posted. What DME to demand from the hospital before you leave — because getting it after discharge means days of phone calls and insurance battles.
- DME Reference with Prices — because nobody tells you the walker requires a referral from a doctor who already left for the day. A plain-English guide to Durable Medical Equipment: what each item does, which ones insurance typically covers, what to request from the hospital versus buy independently, and approximate price ranges.
- Provider Contact Organizer — because the hospital buries every important number across 15 pages of small print. A structured one-page sheet for every number you'll need in the first 72 hours: attending physician, primary care doctor, home health agency, pharmacy, insurance, specialist referrals, PT/OT contacts, and the after-hours escalation number.
- The "Refuse Unsafe Discharge" Framework — because you shouldn't have to choose between being labeled "difficult family" and accepting a dangerous plan. How to formally request a reassessment, put objections in writing on the medical record, demand an occupational therapy evaluation, and use the clinical language that forces administration to respond with procedure instead of pressure.
- Red-Flag Symptom Tracker — because a blank vitals log doesn't tell you which readings are dangerous. A daily log designed around the symptoms that predict readmission: fever trends, wound changes, weight gain (heart failure), new confusion, breathing changes, pain escalation. Each symptom includes the threshold that triggers action and the specific action to take.
After Using This Guide, You'll Be Able To:
- Challenge an unsafe discharge using the exact legal mechanisms available in your country — not by arguing emotionally, but by filing the formal appeals and invoking the specific rights that force the hospital to respond with procedure instead of pressure
- Audit the medication list line by line before leaving the hospital — catching the duplicates, conflicts, and missing medications that cause 40% of post-discharge adverse events
- Set up the first 72 hours at home using a structured protocol — vitals monitoring, medication schedule, symptom red flags, and decision trees that tell you exactly what to do at 2 AM when something doesn't look right
- Demand the training, equipment, and home health support the hospital is legally required to arrange before discharge — and know what to say when they claim "that's not our responsibility"
- Recognize the billing traps — observation status, denied SNF coverage, uncovered DME — before they become surprise bills
- Communicate with the medical team as a documented, respected advocate — using clinical terminology and formal escalation language that gets results instead of dismissals
Why Not the Free Checklists, the Etsy Planners, or the 300-Page Books?
Medicare's official discharge checklist tells you to "ask about complications." It doesn't list which complications to expect based on your parent's condition, what the danger thresholds are, or what to do when the nurse can't answer your question. It tells you to "discuss medications" without mentioning that over half of discharge summaries contain errors. It was written by the hospital's legal team so that when something goes wrong, they can point to the paperwork and say "we told them."
The $3-$5 Etsy planners give you beautifully designed blank pages — medication logs, blood pressure trackers, daily care grids. They assume you already know what data to record, what readings are dangerous, and who to call when something goes wrong. A blank blood pressure log without a threshold that tells you "above 180 systolic, call the doctor immediately" is a decoration, not a safety tool.
The 300-page caregiving books are comprehensive and valuable — for someone with weeks to prepare and the cognitive bandwidth to read a narrative. You are sitting in a hospital room at 11 PM being told your parent leaves tomorrow morning.
This guide is , instant download, and printable. Print the appeal scripts before the discharge meeting. Bring the medication audit to the pharmacy. Tape the decision-tree flowcharts to the refrigerator. Hand the 72-hour protocol to the family member taking the first overnight shift. The format is the feature — it turns a medical crisis into a managed project.
A Readmission Costs Thousands. This Guide Costs .
Accept an unsafe discharge and the math is brutal: a return trip to the ER within 72 hours. Another round of tests. Another hospitalization. More lost wages. More physical decline that never fully recovers — because every readmission takes a piece of the patient's baseline function that doesn't come back. Hiring a private patient advocate to negotiate on your behalf costs $150-$250 per hour. Accepting the first nursing home the discharge planner suggests can lock you into $8,000+/month in facility fees. For , you get the Discharge Defense System to protect your parent yourself — instantly.
The best time to have this guide is before the discharge meeting. Before the 24-hour notice. Before you're standing in a hospital hallway being told "the bed is needed." When you can read the scripts, print the worksheets, and walk into that meeting prepared — not panicked.
Clarity for
Compare it to:
- A private patient advocate consultation: $150-$250/hour
- An ER readmission within 30 days: thousands in copays, deductibles, and lost wages
- Accepting a nursing home placement in a panic: $8,000+/month in facility costs
- A medication error from an unaudited discharge summary: a preventable trip back to the hospital
30-day money-back guarantee. If this guide doesn't give you the scripts, protocols, and confidence to advocate for a safe discharge, you pay nothing.
This guide is an educational resource for families navigating hospital discharge transitions. It is not medical, legal, or financial advice. Always verify current regulations through your country's official healthcare regulatory body and consult with qualified professionals for decisions about specific medical care.
The discharge planner has a clipboard and a quota. You need a Discharge Defense System. Get the Hospital Discharge Guide now and turn the most dangerous transition in modern healthcare into a managed, documented, defended process.